
Am I suitable for TEER?
TEER is a low-risk option suitable for some but not all patients. Studies have shown that in certain patient groups it is less effective than conventional surgery although it can be undertaken at lower risk. Consequently, TEER is usually offered to suitable patients in whom surgery is too high risk or high risk. Suitability will also depend on the anatomy of the mitral valve. Features that might make TEER less suitable include: narrowing or calcification (thickening) of the valve, a complex mechanism of leak, infection of the valve and previous valve surgery or replacement. If it is felt that TEER could be an option, we will need to perform or review your transthoracic echo (TTE) and probably a transoesophageal echocardiogram (TOE scan). If accepted for TEER, we will usually be able to offer the treatment within 4 weeks. Admission is usually on the day of the procedure which is performed under general anaesthetic and takes somewhere between 1 and 2 hours. You will normally be in hospital for 2-3 days and you be able to mobilise on the day after the procedure.
What are the risks of TEER?
TEER with either MitraClip or Pascal is a safe procedure and is normally associated with an overall procedural risk of 1%. This risk will be discussed in detail with you and could be higher or lower than this, depending on your age and the presence of other medical problems. Other risks of TEER include: tamponade (bleeding around the heart which is usually safely treated at the time) 1%, stroke 1%, serious bleeding requiring blood transfusion 2-3%, failure of the procedure to significantly reduce the leak 5%. From our own experience in over 500 patients, more than 90% of patients notice an improvement in symptoms.

How is the procedure performed?
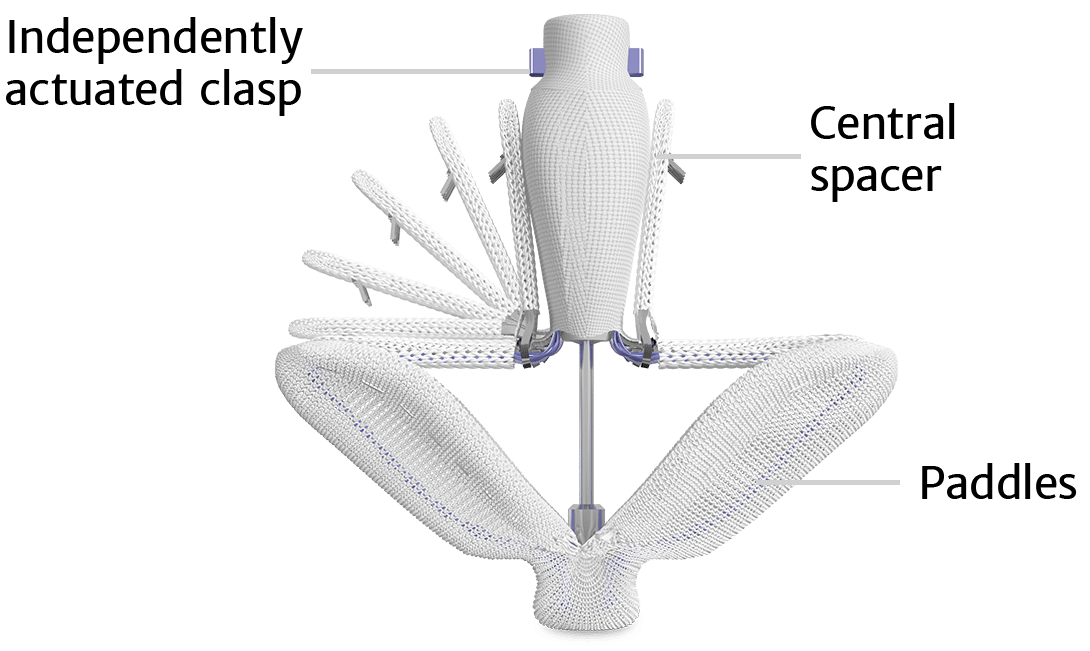
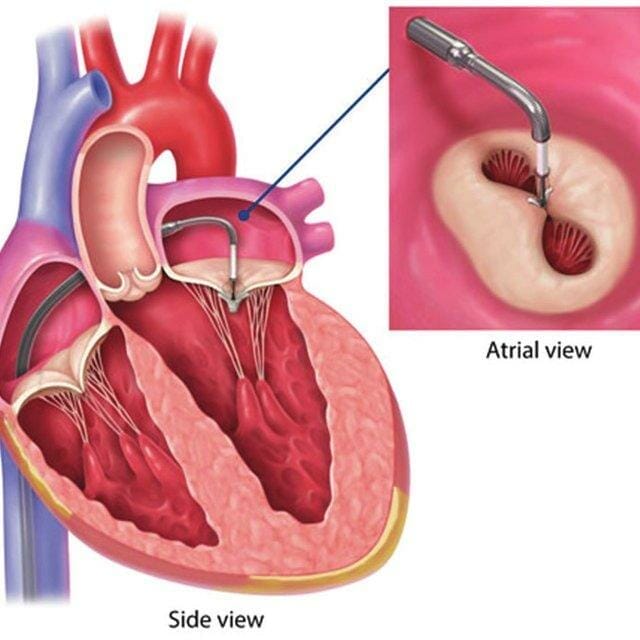
TEER is performed under general anaesthetic. It is undertaken on a ‘beating heart’ without needing to go onto a bypass machine. The procedure is guided throughout by transoesophageal echo (TOE – an echo scan where the probe is passed into the food pipe once you are asleep). A small puncture is made in the groin and a tube is passed into the femoral vein. Guided by XRAY and the TOE, the doctor will make a small hole in the wall between the right and left side of the heart (a transeptal puncture). The TEER guiding catheter is then slowly advanced into the left atrium and towards the mitral valve. The clip (either MitraClip or Pascal) is advanced across the valve and is attached at the point of leak. Multiple clips can be attached if needed. The reduction of mitral regurgitation is assessed in real time and the clip can be detached if the not effective.
The guiding catheter is then withdrawn from the left atrium and removed from the groin. The puncture site is usually closed with a small internal plug (a suture or plug that will dissolve and not need to be removed at a later date). In the majority of cases, the patient is woken up immediately and taken to the ‘recovery’ area. They may spend one night in the high dependency ward, depending on their other medical issues, but usually will return to the general ward on the same day. Patients are reviewed immediately after the procedure and the following day. A transthoracic echo scan (TTE) will be performed to assess the result of the procedure. Patients are usually discharged the following day if well.
Our Team





- Randomized Comparison of Percutaneous Repair and Surgery for Mitral Regurgitation: 5-Year Results of EVEREST II. Feldman T, Kar S, Elmariah S, Smart SC, Trento A, Siegel RJ, Apruzzese P, Fail P, Rinaldi MJ, Smalling RW, Hermiller JB, Heimansohn D, Gray WA, Grayburn PA, Mack MJ, Lim DS, Ailawadi G, Herrmann HC, Acker MA, Silvestry FE, Foster E, Wang A, Glower DD, Mauri L; EVEREST II Investigators. J Am Coll Cardiol. 2015 Dec 29;66(25):2844-2854